Download and print as a PDF (234kB pdf)
What is colpocleisis?
Colpocleisis is an operation to correct prolapse by closing the vagina. It will not be possible to have vaginal sexual activity after that. This will be discussed with you beforehand and only carried out with your voluntary agreement. Other forms of intimacy will remain unaffected.
These operations can be carried out under general, spinal or local anaesthesia.
Why do I need this kind of surgery?
This kind of surgery is done to improve pelvic organ prolapse, which entails slipping down of the vagina, the womb and/or the top of the vagina after hysterectomy.
This prolapse is caused by weakness of the supports that keep the vagina and uterus in place. This weakness can result from a number of factors, such as child bearing, going through the change or weak ligaments and muscles.
The condition can cause a sense of bulge, discomfort, urinary and bowel problems and sexual difficulties.
What can I expect before the operation?
You will be invited for pre-op assessment, when the nursing staff will go through your hospital stay and explain your operation. On admission, the nursing staff will go through your stay on the ward again to ensure you feel comfortable whilst in the hospital.
Please do let us know about any concerns you have or if there is any information you think we should know about that will make your stay with us more comfortable.
You will need to make arrangements for your family, children or any other commitments that you have prior to coming in to hospital and to cover the length of your recovery.
You will see an anaesthetist and the doctor performing the surgery before you go to theatre. It is not unusual to feel anxious; the nursing staff will gladly discuss how you are feeling and talk you through your emotions.
If you have not already signed the consent form in outpatients clinic when your operation was agreed and booked, the doctor will go through it with you before you go to theatre.
You will be asked for permission to enter your data on the national database for continence and prolapse surgery. This is a quality control measure to compare the safety and effectiveness of such procedures at the hospital against other units in the country.
You will be given a quality of life questionnaire to complete and bring with you as you attend for follow up after surgery. This will help us to assess the benefit of surgery for you.
What does the operation involve?
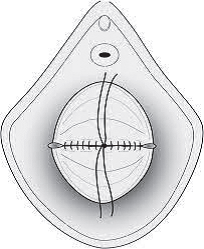
The operation is done through the vagina. Vaginal removal of the uterus and any other procedure for prolapse may be carried out first. After that, the front and back walls of the vagina are then sealed together with sutures.
A catheter may be inserted in the bladder, to save you the need to go to the toilet until you are mobile.
What are the risks?
There are risks with any operation but these are small. The main risks associated with these operations are:
Common risks:
- Initial difficulty in passing urine. This is usually managed by leaving the catheter to drain the bladder for few days. You can still go home and the catheter can be drained into a bag that can be placed on the leg, using a special bandage. This is called a leg bag, which can be emptied in the toilet discretely. It will enable those who need to go home with a catheter to be mobile despite having the catheter. Patients are then seen on the ward for another trial without catheter, when the majority do succeed in passing urine
- Postoperative pain
- Urinary tract infection, which may need antibiotics
- Wound infection, which may need antibiotics
- Wound bruising and delayed wound healing
Uncommon risks:
- Damage to the bladder and/or bowel, which will be repaired at the time of the operation. If such injury is not identified and repaired at the time, there is a risk of fistula, but this is extremely rare
- Venous thrombosis and pulmonary embolism (blood clot in leg/lung). These are reduced by elastic stockings and injections that thin the blood to prevent clots
- Whilst the operation may improve the sense of bulge, there is small chance that urinary, bowel and/or sexual problems may persist. It is hoped however they will at least improve to some degree
- Unmasking of stress incontinence of urine that was hidden by the kink of the urethra, associated with prolapse. This will need assessment and will be managed by pelvic floor muscle training. Surgery might be required, if there is inadequate improvement on pelvic floor muscle training
- Failure and recurrence. This may need further surgery
- Bleeding requiring blood transfusion
- Return to theatre e.g. because of bleeding
In order for you to make an informed choice about your surgery please ask one of the doctors or nurses if you have any questions about the operation before signing the consent form.
What can I expect after the operation?
As you come round from the anaesthetic you may experience episodes of pain and / or nausea. Please let the nursing staff know and they will assess you and take appropriate action.
You may have a catheter in the bladder to save you having to go to the toilet.
You will have a drip to give you fluids, though you will be able to eat and drink. It is not unusual to experience lower back pain and a feeling of fullness in your bowel and generalised discomfort when sitting.
We use a pain score to assess your pain: 0 to 10: 0 = No Pain, 10 = Very Strong Pain.
Your nurse will be checking your blood pressure, pulse, respirations and temperature and monitor any vaginal bleeding. S/he will also ask you to move from side to side and to do leg and breathing exercises once you are able, this will help prevent any pressure damage, a DVT (deep vein thrombosis) or chest infection.
Day 1 after the operation
The drip and catheter are usually removed the next day. The nursing staff will assist with washing as necessary and encourage early mobilisation. We would normally expect you to sit out of bed and begin to walk around the day after your operation.
You will be able to go home when you are passing urine without difficulty. This can be on the first day or later, depending on the how you feel.
You will be asked to pass urine in a jug and will have a scan to measure how much urine is left in the bladder. It is best to forget that you need to pass urine and drink and walk as you would normally do. This helps your bladder to work as normal.
Day 2 after the operation
You will be able to shower and mobilise around the ward on the second day of your operation. It may be painful to open your bowels at first. You will have mild laxatives to soften the stools and prevent constipation and straining.
What about going home?
You will be seen and assessed the following day to check on your recovery and decisions will be made about your care, this information will be shared with you. You may then be able to go home. Please feel free to ask questions about your operation and recovery at any time.
The average length of stay following this kind of surgery is 1 to 2 days.
As you physically recover from your operation, the nursing team will discuss your convalescence. To ensure you have a good recovery you should take note of the following:
What about follow up?
You may be invited for follow up, usually about 12 weeks after surgery.
During this follow up appointment, your symptoms will be reviewed and you will be examined to assess wound healing.
If you have problems before this you can either contact your doctor or contact the hospital to bring the appointment forwards.
Are there any alternatives to this kind of surgery?
You will have been offered vaginal pessaries before being offered surgery.
Alternative procedures include:
- Vaginal repair, without obliterating the vagina. This approach preserves sexual function
- Operations through abdominal (open tummy) or laparoscopic route. These operations include sacrocolpopexy for patients who had previous hysterectomy and sacrohysteropexy as well as utero-sacral suspension for patients who wish to keep it
These can be discussed with your doctor. Patient information leaflets are available for these alternatives.
Who can I contact with any concerns or questions?
You should contact your doctor or the hospital if you notice increased temperature, wound swelling and/or pain, smelling discharge either from the wound or the front passage, blood in urine or motion, abdominal distension and/or failure to open your bowel.
If you have any problems or questions, you can contact:
Lewes Victoria Hospital
![]() Urogynaecology Unit
01273 474 153
Ext. 2178
Urogynaecology Unit
01273 474 153
Ext. 2178
![]() Monday to Friday
9:00 am to 5:00 pm
Monday to Friday
9:00 am to 5:00 pm
Princess Royal Hospital
![]() Gynaecology Ward
01444 441 881
Ext. 5686
Gynaecology Ward
01444 441 881
Ext. 5686
Royal Sussex County Hospital
![]() Gynaecology Ward
01273 696 955
Ext. 4013
Gynaecology Ward
01273 696 955
Ext. 4013
Secretary at Worthing
![]() 01903 205111
Ext. 84811
01903 205111
Ext. 84811
Secretary at St Richard's
![]() 01243 788122
Ext. 32972
01243 788122
Ext. 32972
References/useful links:
British Society of Urogynaecology leaflet: colpocleisis
International Urogynecological Association leaflet: Colpocleisis
This information is intended for patients receiving care in Brighton & Hove or Haywards Heath.
The information here is for guidance purposes only and is in no way intended to replace professional clinical advice by a qualified practitioner.