Download and print as a PDF (248kB pdf)
What is endometriosis?
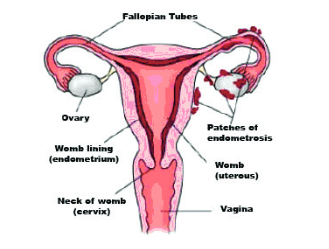
Endometriosis is a very common condition found in women where cells typically found inside the uterus (womb) are located outside of the uterus and surrounding pelvic area including; pelvis, ovaries, fallopian tubes and occasionally the bladder and bowel. Every month these cells react in the same way to those inside the uterus building up then breaking down to bleed which inside the uterus is known as menstruation (period). Although, unlike periods, endometriosis has no way to escape; therefore leading to inflammation, pain and the formation of scar tissue.
Who gets endometriosis?
Endometriosis can affect any females who have started their periods. One in ten women of child bearing age have some degree of endometriosis with symptoms presenting themselves between the ages of 25 to 40 years old. It is estimated that two million women in the UK have this condition.
What causes endometriosis?
The cause for this condition remains unknown. Retrograde menstruation is a possible explanation and this is where some of the blood shed from the womb during your period travels down the fallopian tube or back tracks. Though some professionals feel this condition could be hereditary (runs in the family).
What are the symptoms of endometriosis?
Some women can experience all of the symptoms below, some of them or none at all.
Common Symptoms:
- Pain before a period begins
- Pain during a period
- Pain during sexual intercourse
- Heavy periods
- Rectal symptoms/pain: particularly when opening your bowels
- Infertility: difficulties in becoming pregnant
- Back pain
- Pelvic pain
Uncommon Symptoms:
- Pain in the lower abdomen: particularly when passing urine
- Blood in your urine or faeces
- Fatigue
- Endometriosis can be found in other areas of the body causing pain when your period is due and throughout
How is endometriosis diagnosed?
Endometriosis can be difficult to diagnose immediately as the symptoms experienced are similar to those of other conditions, an example being irritable bowel syndrome.
A formal diagnosis of endometriosis is made through performing a diagnostic laparoscopy (keyhole surgery). This usually is a day case procedure, performed under a general anaesthetic (putting you to sleep) where a small camera is inserted into your belly button to look inside the abdomen and pelvis.
The diagnosis of this can then be made by the doctor sometimes just by visualising the endometriosis. Often a small piece of endometriosis known as a biopsy is sent for testing with results relayed to you when they are back. If fertility has been a concern then the doctor may also flush your tubes to make sure they are clear and patent checking for any blockages/signs of endometriosis.
How can endometriosis progress?
Untreated endometriosis becomes worse in approximately four out of ten women; however in about three out of ten women it will improve. For the remainder the condition and symptoms remain the same. Women with severe untreated endometriosis are at risk of complications such as; obstruction or blockage of the ureter (the tube between the kidney and bladder).
Can endometriosis be treated, and how?
Treatment is not required if there is no pain and fertility is not an issue. Mild endometriosis evident during a diagnostic laparoscopy may be treated at the same time.
In more severe cases there are many options available and these are divided into medical management and surgical management. The option that is best for you will be discussed with your doctor and will depend on personal individual factors including: age, pregnancy status and thoughts on future pregnancies, how you feel about undergoing surgery, how effective previous treatment has been and what symptoms you want to try and manage.
Medical Management
The combined oral contraceptive pill
This does not make endometriosis disappear but may mask symptoms experienced by usually lightening the blood flow and reducing pain experienced when having a period. This is temporarily done by preventing ovulation. This management is usually effective in managing symptoms such as pain and heavy periods.
Intrauterine system (mirena coil)
This is a T shaped device that is inserted into the womb via the cervix and shaped in that particular way to fit into the lining of the womb. Having a coil inserted is an option to managing heavy periods as one in five women with coils stop having periods all together due to the fact the hormone being released by the coil thins the lining of the womb. The coil can be inserted as an outpatient/at the GP surgery, acts as a contraceptive and lasts for five years. Adenomyosis (this is where endometrial tissue which normally lines the womb is found growing into the muscular wall) is another reason how the coil device can help symptoms of endometriosis.
Depo Provera
This is a progestogen administered as an injection every three months. Progestogens are hormones and the injection works by stopping your periods whilst having the injections.
GNRH Analogues
This is an injection and works by stopping your ovaries from producing the hormone oestrogen. It mimics a temporary state of menopause and has shown to be effective in reducing the deposits of endometriosis found outside of the womb. Sometimes if having an operation is an option the doctors might recommend this treatment prior to the operation date as they want to shrink as much as possible so minimal pelvic tissue is excised. This treatment will only be used for a maximum of six months as the side effects can be unpleasant. The doctor will go through these with you when discussing options.
Surgical Management
Keyhole surgery
This will involve being put to sleep and through small incisions in your abdomen your endometriosis will be destroyed or endometriotic tissue cut out to try and restore normal pelvic anatomy where possible. This treatment often reduces pelvic pain and improves fertility rates.
Hysterectomy (+/- Bilateral Salpingo oophrectomy BSO)
This involves removing the womb, fallopian tubes and often ovaries. This operation is not a guaranteed way to make you pain free as you may still have evidence of endometriosis on your bladder and bowel, organs which are not removed as part of this surgery. This operation should only be considered in women who are certain they have no further plans to become pregnant and where other previous treatment has been tried and failed. Your tubes and ovaries may be removed at the same time.
What are the risks?
Medical Management
These will be discussed thoroughly between you and your doctor prior to commencing treatment although some risks associated with choosing medical management are:
- May not be effective
- Will not remove endometriosis
- May be contraindicated in women who wish to become pregnant
- May reduce long term fertility
- Side effects of individual drugs with a high non-compliance rate
Surgical Management
The risks depend on the operation performed but they may include:
- Post operative pain: particularly shoulder tip pain if performed keyhole
- Urinary infection, retention/or frequency
- Wound infection, bruising or delayed healing
- Damage to the bladder/or bowel
- Pelvic abscess of infection
- Venous thrombosis or pulmonary embolism (clot in leg/lung)
- Keyhole surgery converting to open incision
- Failure to gain entry to abdominal cavity and complete the procedure
- Hernia at the site of entry
- Haemorrhage requiring blood transfusion
- Unexpected return to theatre
In order for you to make an informed choice about your operation please ask one of the doctors or nurses if you have any questions about the operation before signing the consent form.
Can I have children if I have endometriosis?
Many women who have endometriosis are able to have children without any problems although some women will find conceiving more difficult. Severe endometriosis may mean adhesions present around the ovaries and this can prevent the egg from moving down the fallopian tube to conceive.
With the difficulties of getting pregnant endometriosis have treatments which may help (see listed below).
You can still get pregnant if you have severe endometriosis, it could just take longer.
Are there any alternative treatments to treat endometriosis or help manage symptoms?
Complementary therapies have not been scientifically proven but many women feel that therapies such as acupuncture or reflexology help to manage symptoms.
Pain control is better if you are able to stay ahead of it by taking medication regularly. Anti inflammatory drugs (Ibuprofen, Nurofen) provide good pain control and can be taken with paracetamol and/or codeine.
Exercise is a good relief for pain symptoms and this can be whatever exercising you are most comfortable with doing. Irritable bowel syndrome and endometriosis co exists and can be managed by following a healthy diet with plenty of fruit and vegetables. Peppermint water may also help too.
Who can I contact with any concerns or questions?
If you have any problems or are worried, please do not hesitate to contact us on the gynaecology ward:
Princess Royal Hospital
![]() Horsted Keynes Ward
01444 441881
Ext. 65686
Horsted Keynes Ward
01444 441881
Ext. 65686
Royal Sussex County Hospital
![]() 01273 696955
Ext. 4013
01273 696955
Ext. 4013
This information sheet has been produced by the Gynaecology Ward Sister Hannah Tompsett and Samantha Backley.
This information is intended for patients receiving care in Brighton & Hove or Haywards Heath.
The information in this leaflet is for guidance purposes only and is in no way intended to replace professional clinical advice by a qualified practitioner.