Download and print as a PDF (1MB pdf)
What is this information about?
This information is about hip fracture (a broken hip bone) and the care that you will receive in Broadwater Ward, Worthing Hospital after you have had a hip fracture.
Why have I been given this information?
You have been given this information because you have had a hip fracture or are a carer or relative of someone who has. Reading this information will help you to:
- understand what it means to have had a hip fracture
- know what to expect from your stay in hospital, your treatment and your rehabilitation (rehab)
- know what you can do yourself to aid your recovery
- understand what will happen when you leave hospital after your stay (when you are discharged from hospital)
- know where to find further help and support.
Following the advice in this information can help you to heal as quickly and well as possible.
If there is anything in this information you do not understand or would like to know more about, please ask any member of the multi-disciplinary team (MDT). This is the team made up of Doctors, Nurses, Care Workers, Occupational Therapists, Physiotherapists and Pharmacists who will be providing your care. They will be happy to help.
Where will I stay while I am in hospital?
You are likely to spend most of your stay on Broadwater Ward, Worthing Hospital. Some people may have to spend time on another ward.
Wherever you receive your care, you will be cared for by a team of specialists.
How can I contact Broadwater Ward?
Phone: 01903 205 111 ext. 85797, 84906 or 85517
How can I recognise the different staff groups who make up the MDT on Broadwater Ward?
You can identify the different members of the MDT from their uniforms using the illustration below:
How can I contact Broadwater Ward?
Phone: 01903 205 111 ext. 85797, 84906 or 85517.
What are the visiting times?
Visiting time is from 2pm to 8pm every day with a maximum of 2 visitors at the same time for each patient.
If you need to make different arrangements for visiting do discuss this with the nurse in charge or ward manager before your visit.
We understand how important the support of family and friends is but please be aware, people who have had a hip fracture can get tired very easily.
Be mindful of how often you visit your relative or loved one and how long your visits are as they may find visits tiring. It is important that they get the care, therapy and rest periods that they need.
What is a hip fracture?
A hip fracture is a crack or break at the top (head) of the thigh bone (femur) close to the hip joint. They often happen because of a fall.
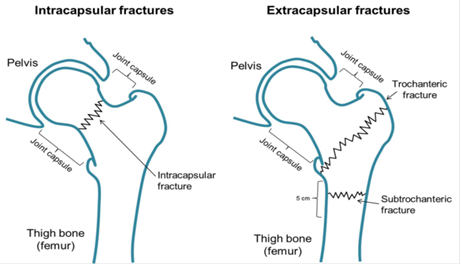
There are two main types of hip fracture:
- intracapsular fracture. This is when the ‘ball’ at the head of the thigh bone has broken off the thigh bone.
- extracapsular fracture. This is when the break is further down the thigh bone and outside of the hip joint.
Most hip fractures need an operation to fix them. If we think you have had a hip fracture, we usually do an X-ray to confirm this.
The type of operation you need depends on:
- where the break or crack is on your thigh bone
- your age
- if you use any walking aids such as a zimmer frame or walking stick
- the distances you usually walk (your exercise tolerance).
What are the four main types of hip operation?
1. Hemiarthroplasty
This is used when the head of the thigh bone is fractured (an intracapsular fracture).
The head of the thigh bone is replaced with a metal ball and stem, but the socket of the hip joint stays the same and is not replaced.

2. Total hip replacement
This is used when the fracture is in the head of the thigh bone and the hip socket (an intracapsular fracture).
The head of the thigh bone is replaced with a metal ball and stem and the hip socket is replaced with a plastic cup.
3. Dynamic hip screw
This is used when the fracture is outside of the hip joint (extracapsular)
The bones are put back into the correct position and fixed together with a plate and screw.
4. Intramedullary nail
This is used when the fracture is outside of the hip joint (extracapsular) and is further down the thigh bone.
A metal rod goes through the middle of the bone and is held together with screws.
How soon after my operation will I be able to bear my weight on my hip and start standing and walking?
You will usually be able to fully bear your weight on your hip and start standing and walking on the day after your operation for all four of these operations.
Does everyone with a hip fracture have an operation to fix it?
No. A decision will be made not to operate on you if an operation is not the right treatment for you. This is usually if:
- you have an ‘impacted’ hip fracture where the bones are in a good, stable position and should heal over time
- the hip fracture happened a few weeks ago and has already started to heal
- there are concerns that you may be too frail or unwell to cope with surgery.
The treatment you may get for your hip fracture if an operation is not right for you is called ‘conservative treatment’ or ‘non-hip surgery treatment’.
If you are unable to have an operation you may be given pain relief via a tube to numb the area of your injury.
Your Orthopaedic Consultant (bone specialist) will decide how much weight you can put through your hip joint.
If you are having conservative treatment, some of the contents of this information will not apply to you. If you are unsure do ask the members of the multidisciplinary team what is relevant for you and what is not.
During your hospital stay
How soon after I have come into hospital (been admitted) am I likely to have my operation?
We aim to do your operation as soon as possible. For most people this will be within 36 hours (a day and a half) of being admitted to hospital.
What happens before my operation
We aim to admit you from A&E directly to Broadwater Ward.
- The staff will get you ready for your operation by:
- taking a small amount of your blood for blood tests
- measuring how fast your heart is beating and the way it is beating using an ECG machine
- putting in a cannula (a fine tube that goes into a vein), usually in your arm or the back of your hand. We use the cannula to give you medicines straight into your bloodstream.
- asking you to tell us your weight and height if these were not measured when you came into hospital.
- An anaesthetist (specialist in giving you medicine to make sure that you are drowsy, ‘asleep’ or will be numb so you do not feel pain during your operation) will see you to check whether you are fit and well enough to have your operation.
- We may put in a urinary catheter. This is a bendy tube used to empty your pee (urine) from your body and collect it in a drainage bag. We may do this before you go into the room where you will have your operation (the operating theatre) or when you have got to the room.
We aim to remove your catheter within a few days after your operation.
After your operation
When you have recovered from your anaesthetic you will be taken back to the ward. You may be moved to another part of the ward while you continue to recover and have therapy and treatment.
During your stay doctors who are specialists in treating older people with broken bones (Ortho-geriatric doctors) will see you to check how you are.
Medicines
We will offer you medicine to control your pain (pain relief) at regular times. You can ask for more if you need them.
It is important that you start to walk and move around (mobilise) as soon as you can after your operation. Having pain relief before you get out of bed to do your physiotherapy sessions can help you to do them.
We usually give most people antibiotics after their operation to help to prevent them from getting an infection.
Mobilising (getting out of bed, moving around and walking)
We will aim to get you out of bed and sitting in a chair the day after your operation. It helps you to be independent and to recover if you get up and dressed in your clothes each day. We will encourage you to do this.
Walking as soon as possible after your operation aids healing and can help to prevent things going wrong (complications) with your recovery.
Eating after your operation
It is important for you to eat well while you recover as this aids healing, but many people do not feel hungry (have a small appetite) after their operation. We may give you high-calorie drinks to sip in between meals to help you to get the nutrition you need to recover. These ‘nutritional supplement’ drinks are called Fortijuice and Fortisips Compact. If we give you these drinks, try to have them as they can help you to recover.
If you remain underweight (your Body Mass Index (BMI) is under 20) we may refer you to a Dietitian. They will help you to get the nutrition you need to help you to recover.
What problems can happen after a hip fracture?
A hip fracture is a very serious injury. It can even be life threatening for some people. Some people do not survive their stay in hospital and some people’s health gets worse after they leave hospital.
Having a fracture is often a sign that your health is not good and that it may get worse in the short or longer term.
Complications and side effects that you could get after a hip fracture include:
- Constipation. Many people get this after an operation. It can be made worse by:
- not moving around so much
- side effects of the medicines you are taking
- not drinking enough (being dehydrated)
- a change in what you are eating and drinking (your diet)
- being somewhere that you are not familiar with.
We will offer you laxative medicine to help you to poo (have a bowel movement). Drinking more fluids can also help if you have constipation.
- Confusion (delirium). Many people have this after an operation. Confusion can be distressing for you and your relatives. There is a higher chance that you may get confusion or feel disorientated (for example, you do not know where you are or what time it is) if you have had short term memory problems or have dementia.
Confusion after your operation can be made worse by:
- medicines that you have had such as pain relief or anaesthetics
- having an infection
- having a low level of oxygen in your blood
- being somewhere that you are not familiar with.
Confusion is often worse in the evenings. If you have confusion your relatives should speak with nursing staff. They can tell your relatives about ways to help you. This could include making sure you know where you are and what is happening and bringing items that you are familiar with into hospital.
- Bleeding. You may lose blood during your operation. If you do, you may need a blood transfusion or to take iron tablets.
- Chest Infection. Because you are not moving around as much you are more likely to get a chest infection such as pneumonia. If you do, it is likely that we will treat it with antibiotics.
- Diarrhoea (watery poos). Some of the medicines which you will be taking can upset your bowels and cause diarrhoea. If you are taking antibiotics there is a greater chance that you may get diarrhoea caused by the clostridium difficile (c. diff) germ. Sometimes there are seasonal outbreaks in hospitals of illnesses that cause people to be sick (vomit) and have diarrhoea in hospitals.
We will do everything that we can do help to make sure that you do not catch a germ that will give you diarrhoea and vomiting and to treat you if you do.
- Leg swelling. Many people get this in the leg that has been operated on. It can last for several months. It usually improves as you return to moving around more.
Try to raise your leg (for example by resting it on a stool) when you are sitting down as this can help. But, you must also give your leg a chance to bend and encourage movement.
Be aware
If your leg becomes hot, red (this may look different on black or brown skin) or gets more painful do let a member of staff know straight away. These can be symptoms of an infection or blood clot.
- Dislocation. It is rare for your hip joint to become dislocated after you have had one or both halves of your hip joint replaced (hemi-arthroplasty or total hip replacement). If this does happen, you will need another operation to put your new hip prosthetic (metal) joint back into the right position.
- Pressure sores. Many people who have a hip fracture also have fragile skin. There is a greater chance that you may get pressure sores if you are not moving around much or getting enough nutrition. These are often on your heels or your bottom. Pressure sores can be painful and allow germs to get into your body where your skin is broken.
Nursing staff will check often to see if you are getting a pressure sore from as soon as you arrive on the ward. They will ask you to change your position often when you are laying or sitting down as this helps you to avoid getting pressure sores.
- Fall in hospital. Breaking your hip means that there may be a greater chance that you will have falls in future. Being in hospital, not being familiar with what is around you, and having a painful and weak leg also makes it more likely that you may fall.
Research has shown that when hospital staff work together, they can reduce falls by 20 to 30%. You and your family can also help by being aware of the risks and the actions you can take, as well as talking to the people looking after you about falls prevention. You can find further information in our Preventing falls in hospital leaflet.
- Wound Infection. To make it less likely that you will get a wound infection we:
- give you a specialist wash before your operation. This kills germs which could get from your skin into your wound.
- give most people antibiotics
- check your wound for any signs of infection. Most people do not need further treatment.
- leave your wound dressing on for five to seven days.
- Blood clots (Deep Vein Thrombosis ‘DVT’) or Pulmonary Embolism ‘PE’)
Some people get a blood clot in a vein in their lower leg (calf) after a hip fracture. This is called a DVT.
Rarely, a clot breaks away from where it is in your leg and travels through your bloodstream to the lungs. This is called a PE. Blood clots can be painful and dangerous. Some people die because of a blood clot.
Not moving around much, not drinking enough and having other health conditions can all make it more likely that you may get a blood clot.
To reduce the likelihood of you getting a blood clot we will give you an injection of medicine that thins your blood each evening. We will also give you ‘Flowtron’ pumps to wear on your lower legs. These squeeze your legs enough to increase your blood circulation and so reduce the chance of clots.
If you need to take medicine yourself (self-administer medicine) to reduce the chance of getting a blood clot we will teach you how to do this.
- Your hip joint repair has not worked as it should (failure of fixation). This does not happen often, but sometimes, over time, the ‘metalwork’ in your new joint can move into the wrong position. If this happens you may need another operation to fix it.
- Your operated leg is not the same length as it was before your operation (leg length discrepancy). Your leg could be longer or shorter than it was before. Any difference is likely to be small. Your spine may adapt to it so that you do not notice any difference at all. If you notice a difference, you may need a ‘shoe raise’ from around six weeks after your operation.
Will you share any information about me and my treatment?
Hospitals that treat patients with a hip fracture send information (data) to the National Hip Fracture database (NHFD). This helps to improve care for people with hip fractures nationally. The public can see this data at www.nhfd.co.uk . When the data is published no one can tell that it is about you. It is ‘anonymised’.
What other treatment might I get during my stay?
- Brittle bone (osteoporosis) treatment. If you are female and over 60 or male and over 65 and have a broken hip, you may have a condition known as osteoporosis or brittle bones.
Many females of this age have osteoporosis. If we think you may have it, we will refer you for a special scan called a DEXA scan. Your GP will arrange for you to have this after you have left hospital. If you are over 75 years old, we will give you treatment for osteoporosis straight away without you having a scan. This is because people over 75 are very likely to have osteoporosis.
There are different treatments for osteoporosis. Our doctor may talk with you about giving you ‘bone protection’ treatment. They may give you a dose of a medicine called zoledronic acid while you are in hospital. We give this as an ‘IV infusion’ (a drip) through a very thin tube that goes into a blood vessel, usually on your hand or arm.
You can find further information about osteoporosis on the Osteoporosis Society website or you can phone them: 0808 800 0035.
Be aware
Once you have started treatment for osteoporosis it is likely that you will need to have it for at least five years.
- Treatment of iron deficiency anaemia with intravenous (IV) iron
Your medical team will check your blood test results. Sometimes these show that you do not have enough iron in your blood (you have iron deficiency anaemia). This could be because:
- you have not had enough iron in your diet (what you eat and drink)
- your body cannot take in (absorb) or store iron as well as it should
- you have lost blood, for example, during your operation.
Iron is important because it helps your body to make haemoglobin. Haemoglobin, or ‘Hb’ carries the oxygen in your blood around your body to where it is needed and gives blood its red colour.
Your medical team may suggest you have IV iron treatment. This boosts the iron stored in your body. It is given to you directly into a vein (intravenously) through a small hollow needle. Fluid containing the iron (an iron infusion) flows from a bag. Giving fluid in this way is called giving it by ‘drip’.
IV iron therapy is very safe and works very well. Like most therapies it can have some side effects. These include:
- staining of your skin where the infusion enters your body through the cannula (the infusion site)
- your skin changing colour over all of your body. This may be mild and hard to notice or a darker colour.
- having an allergic reaction to the IV iron infusion. This may not happen straight away but some time later after your infusion.
Be aware
It is important that you read this information leaflet about IV iron infusion. Ask staff if you would like a printed copy.
Once you have read this and staff are sure that you know what an IV iron infusion involves, they will ask you to give your consent (agreement) to having the treatment. If you agree to having the treatment you show this by signing a ‘consent form’.
- Treatment to help prevent blood clots
You will have a daily injection of a medicine called enoxaparin to prevent blood clots. You will also be given Flowtron pumps to wear on your legs. These increase your blood circulation and make it less likely that you will get a blood clot.
Caring for people with dementia
There are many different types of dementia. With some of them, patients find it difficult to retain and recall new information.
This can be made worse when people are in hospital and things, people and places are not familiar to them. This worse state may not get better. It can become a person’s new normal.
We can help with:
- ‘This is Me’ volunteers on the ward. They support patients with dementia by giving them activities and talking with them.
- ‘This is Me Passport’. As part of our care, we’ll ask family members or carers to fill out a ‘This is Me’ Passport. This helps staff understand the patient’s likes and dislikes. It can make care more personal to patients and help them to engage with their care and recovery.
- Carer’s Passport. If you are a relative visiting a patient with dementia, a ‘Carer’s Passport’ lets you visit outside of the usual visiting times. You can get yours from the ward staff. Please ask them for details.
- Physiotherapy for patients with dementia.
This focuses on:
- clear, simple instructions and helping people to do the things they really need to such as getting in and out of bed or onto a commode.
- only teaching people exercises that are right for them if appropriate.
- aiming to get people out of hospital and back to their rest or care home (discharge them) within a week of them being medically optimised for discharge. People with dementia often do better in a place that they know well.
‘Medically optimised for discharge’ means your condition is under control and not getting worse and we have given you all the treatment and tests that you need to have in hospital. We will also make sure your pain is under control before you are discharged.
For many people, when they are feeling ready to move around more, staff at their rest or nursing home can help and support them to do this. We may ask a Community Physiotherapist to visit you if we think that is right for you.
If you have dementia and you are still living in your own home, you may need extra physiotherapy and occupational therapy so that you can do the things that you need to and are safe to do them.
Mobility and rehabilitation
What will the Physiotherapy team do to help me to recover and return, as far as I can, to doing the things I used to before I broke my hip?
The Physiotherapy Team will come to see you the day after your operation. We will create a programme for you to meet your needs. This will include:
- talking with you about how much you were able to move around and do things before you broke your hip
- talking with you about any falls you may have had in the past
- making sure you have enough pain relief
- setting short-term and long-term goals for your recovery with you and what you may be able to do in future
- showing you some basic hip exercises so that you can do them yourself each day
- aiming to support you out of bed and into a chair. We help you to use any equipment that you may need, such as a zimmer frame, to help you to step and move around.
We aim to see you three times a week to:
- help you to walk better
- help build your confidence
- check how you are doing with your hip exercises and help you to move on to the next stage with them
- work with you on exercises to help your balance if you need them.
Over the weekends nursing staff may also help with these things.
We also run:
- a chair based exercise group once a week. This includes a chance for you to talk to other patients on the ward).
- teaching sessions for family and friends so that they can do hip exercises with you when they visit.
What exercises should I do to help my recovery?
Be aware,
- the more you can do in the days soon after your operation to help you get back on your feet, the better the outcome.
- it is important that you practice the exercises below three to four times a day for at least six weeks to help your recovery.
These exercises will:
- improve your muscle strength
- improve how much you are able to move and how flexible your joints are
- reduce the chance that you may get a problem with your circulation


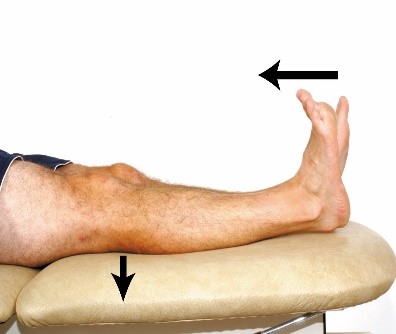



Repeat 10 times.

Sitting. Keeping your knees bent, lift your knee up towards your chest. Lower and repeat on the other side. Repeat 10 times.






Exercises to move on to (progression exercises)


Walking
We will show you how to walk with a zimmer frame and then elbow crutches or walking sticks if, and when, we feel you’re ready. We will also give you:
- tips and advice on how you can walk in as natural a way as possible
- information on how to continue to make progress with your walking when you are at home.
What sequence of movements should I follow when I walk?
- Move your walking aid forward first
- Step forward with your operated leg
- Finally step forward with your non-operated leg.
When you’re walking be aware:
- try not to limp
- bend your knee as you bring your operated leg forwards to take the next step
- take small steps when you turn to change direction.
How should I go up and down stairs?
To go both up and down stairs do:
- take one step at a time
- hold the handrail with one hand and your crutches in the other
- stand close to the stairs
To go up stairs follow these stages:
- Take your first step with your non-operated leg
- Then bring up your operated leg
- Finish the step by bringing up your crutches
To go down stairs follow these stages:
- Place your crutch down onto the step
- Step down with your operated leg
- Step down with your non-operated leg.
How can I return to doing the everyday things that I did before I broke my hip?
It may take time for you to get used to doing everyday activities again. Occupational therapy can help with this.
Your Occupational Therapist (OT) will give you advice about:
- the equipment you might need
- how you can adapt the way you do some activities.
This will help you to be as independent as you can be.
What do I need to know about doing everyday activities?
Washing
It is important for you to practice washing and dressing yourself while you are in hospital.
When you go back home:
- It will not be easy for you to get in and out of the bath after your operation. This is likely to last for a few weeks after your operation. It may also be hard to use a shower if it is over your bath.
- If you have a walk-in shower or shower cubicle at home, you can use this. Your wound dressing is shower proof.
- You may need to ‘strip-wash’ when you first go home. This means that you have a thorough, all-over wash with a flannel or sponge but do not get into a bath or shower. Washing in this way can help you to get back your confidence and be independent.
- To wash your hair, stand and lean over the sink. Stretch your operated leg out behind you. If you can, use the kitchen sink to wash your hair. It is usually higher than a bathroom sink and easier to use.
Your Occupational Therapist may provide you with:
- a perching stool to help you to strip wash
- other equipment to help you to wash, bath or shower if you need it.
Getting dressed
- After your operation, your hip is likely to be slightly stiff and uncomfortable. This may make it hard to bend and put on your underwear, trousers or skirt. If so, you may find it helpful to use small aids such as a ‘helping hand’ or a long-handled shoe-horn.
Ask your Occupational Therapist about these during your stay in hospital.

- Do ask your family to bring in:
- a set of clothes for you to wear in hospital during the day
- your toiletries such as shaving things, a toothbrush and antiperspirant.
These will allow you to practice getting dressed and help you to get back to your normal routine.
- Please talk to your OT If you feel unable to wash and dress without some help. They will suggest options for help that may be right for you.
Cooking
- If you were able to prepare your own meals before your operation, you should be able to manage this when you return home. You may become tired more quickly when standing. If so, it might help to have a stool or chair nearby.
- Think about how your kitchen cupboards are arranged. Make sure it’s easy to reach everything without having to bend or stretch too far.
- If you do not feel confident about cooking, talk with your OT before you go home. They can give you information on meal delivery services and other things that may help.
Carrying
- Carrying food and drink may be difficult as you’re likely to be using a walking frame or crutches. Think about things you can do that will help you. For example, this could be using a bag (such as a rucksack) to carry things. Ask your OT if you would like further advice about carrying things.
Shopping
- You are likely to need help with shopping when you first go home. Before you go home:
- think about who you could ask to help you with your food shopping and arrange for them to help or
- consider ordering your shopping online or having it delivered.
- Ask someone to dispose of out-of-date food that you may have and to buy things such as bread and milk that you will need as soon as you go home.
Furniture Heights
- It’s important that your furniture at home is the right height so you can sit down and get up safely and be more comfortable after your operation.
- Your OT will ask about your furniture and how high it is. Please ask your family to help with this by returning the ‘furniture height form’ we will give them as soon as possible. This helps to prevent any delays in ordering equipment you might need.
Housework
- Avoid heavy tasks such as vacuuming or carrying lots of laundry for up to six weeks. Ask friends or family for help if you need it. Your OT can give you information about other help that may be available to you.
Driving and being a passenger
- You will be unable to drive for some time after your operation. You must not drive again until you can safely carry out an emergency stop with your operated leg. This will usually be at around 6 weeks after your operation but may take longer.
Before you drive again, practice using the pedals in a parked car as if you were doing an emergency stop.
- Let your insurance company know that you have had a hip fracture before you start driving again. Ask them to confirm that you are insured. They may ask for a letter from your doctor to confirm that you are fit to drive. Do not drive until you know you are insured to do so.
- If you are a passenger in a car do:
- use the front passenger seat
- make sure that it is pushed back as far as it will go and is slightly tilted back (reclined).
Follow these steps for getting in and out of the car:
- Consider the height of the car
- Make sure the car is parked so that you are not getting into the car by stepping off the kerb
- Wind down the window and use the door and doorframe to lower yourself into the seat
- Lift one leg in at a time.
Reverse these steps to get out of the car.
Sport and leisure
Please speak with your OT about any activities or hobbies that you are keen to return to. They will be able to advise you on how quickly you can return to doing them. You may need to adapt the way you do things in the short term.
Change of mood
- Some people find they have a change in mood during their stay. Please let a member of the team know if this worries you. We can ask our chaplaincy or volunteer ward services to offer you emotional support.
- It may help to think of activities you can enjoy in hospital and ask family and friends to bring these in. For example, reading, puzzle books, games, watching films on a laptop or tablet or listening to music. It can also help to have familiar things around you.
Sex
- Unless your doctor advises that you should not, you can return to having sex when your wound has healed well and the stitches have been removed.
- The most stable position for your hip is on your back, with your partner on top. Please ask ward staff for an information sheet with further advice and tips for returning to having sex if you would like it.
Pets
- When you return home your pets are likely to be very excited to see you. Consider sitting down when you first meet them again in case they jump up.
- Always be aware of where your pets are when you’re walking so that you do not trip over them.
- You may need to ask family or friends to help you look after your pets while you are recovering.
Work
- You should be able to return to work between 6 to 12 weeks after your operation. Talk with your doctor and OT about when it is best for you to return to work.
- This will depend on the type of work that you do. If you have a manual job (where you do a lot of physical work) it may take longer.
Going home
- We aim to get you home as soon as possible after your operation. We start to plan for this from the time you arrive on the ward.
- If you were very independent and active before your operation you may feel ready to go home in the first week after your operation. You may need support from the Community Physiotherapy Team or other community services. We will talk about this with you.
- If you were less mobile before you came into hospital, it may take you longer for you to recover and get back on your feet. If so, we may therefore offer you a period of rehabilitation at one of our community hospitals.
- Having goals to work towards and being motivated to achieve them is important. It can help you to recover and be able to do the things you want to more quickly.
Be aware, for some patients, rehabilitation takes many months. You may need extra support and equipment to help you manage safely at home in the future.
Frail patients or those with pre-existing medical conditions may find it harder to get over a fractured hip. They may become dependent on others for help with moving around or for daily tasks. This could mean they need to move permanently into long-term care.
It is also possible that these people may die during or shortly after their operation.
When can I go home?
You are usually able to go home once:
- your condition is stable or getting better and we have given you all the treatment and tests that you needed to have in hospital (you are medically optimised)
- you are walking safely with a walking aid, such as a zimmer frame, which is right for you
- you can do your hip exercises on your own or with your friends and family
- you can use any steps or stairs safely if you need to
- you are able to do the everyday things that you need to so that you are safe and comfortable (activities of daily living). If you cannot do these for yourself the support that you need must be in place.
- you have all the equipment you need.

Do you look after someone who could not manage without your help?
If you are looking after a partner, relative, child, neighbour or friend who has long term illness or is disabled or frail, then you are a carer and Carers Support is here to help you.
Please phone 0300 028 8888 to speak to us.
What happens on the day I go home?
The team will try to have everything ready for you so that you can leave hospital on the morning of your discharge.
If you cannot be collected from hospital until later in the day, there is a ‘discharge lounge’ where you can wait. We will arrange for you to be taken there if you need to use it.
There are staff to look after you in the discharge lounge including a nurse who can give you any medicines you need. There are also drinks and snacks available and an accessible toilet.
- Before you leave the ward you will be given:
- a discharge booklet. This has lots of useful information in it such as a phone number for you to contact if you have any questions or problems once you are home.
- equipment on loan to you for use at home such as walking aids or toilet frames
- information on whether you have had internal dissolvable stitches (sutures), steristrips, or clips used to close your wound. If you have clips you will be given a clip remover to take home. The clips should be removed at 14 days after your operation. If you have gone home before your clips or stitches are removed we will refer you to a District Nurse, who will remove them for you.
- a letter for your practice nurse. This tells them when to check your wound. District nurses will only be contacted and asked to check your wound if you are unable to go to your surgery for wound care.
- a copy of your GP letter telling them about your hospital stay.
- spare dressings if you need them.
- Enoxaparin injections (to help prevent you from getting a blood clot) and a yellow sharps box if you need them. This yellow box will be collected free of charge by your local council. Please phone them directly to arrange collection.
- If you are on osteoporosis medication, please remember you need to continue to take it for several years.
Who can I contact if I need further information or support after I have read this information?
If you are in hospital, please speak with the ward staff.
If you have been discharged, please contact your GP surgery or use the online NHS 111 service.
This information is intended for patients receiving care in Worthing.
The information here is for guidance purposes only and is in no way intended to replace professional clinical advice by a qualified practitioner.