Download and print as a PDF (1MB pdf)
Physiotherapy Department
What is this information about?
This information is to help you with your recovery following your operation to repair your anterior cruciate ligament (ACL reconstruction).
It explains:
- what the ACL is
- what a tendon graft (the operation used to reconstruct your ACL) is
- what to expect after your operation
- how soon you can return to activities
- how to care for your operation wound, graft, and health after you go home from hospital
- what follow-up care appointments you will have
- what you should do, and not do during the time that you are recovering
- what goals you should have for your recovery
- what physiotherapy support (including equipment such as a leg brace) you can expect to help you to meet your goals and recover
- what exercises you may do at different stages of your recovery
- who to contact if you need further information or support after you have read this information.
Why have I been given this information?
You have been given this information because you (or a family member or someone you care for) are having an operation to repair your ACL.
Reading this information can help you to know what to expect from your operation and during your recovery. The advice in this information, if you follow it, can help you to:
- recover as quickly and as fully as possible
- stay safe while you recover
What are the most important things that will help me to recover?
- Be confident that following the advice in this information and sticking with your rehabilitation plan and exercises will mean that you maximise your recovery.
- Always work towards your goals for your recovery and what you want to be able to do. You will set these goals along with your physiotherapist.
Be aware
rehabilitation after ACL repair is different for everyone. The amount of time people take to recover and how easy they find it can vary a lot. These can depend on:
– the type of operation you have had
– your general health and fitness before and after your operation
– the goals that you are aiming for.
The timescales mentioned in this information for moving to different stages of rehabilitation are only a rough guide. You should only move on from one stage to the next if you and your physiotherapist feel that you are ready.
What is the anterior cruciate ligament? (ACL)
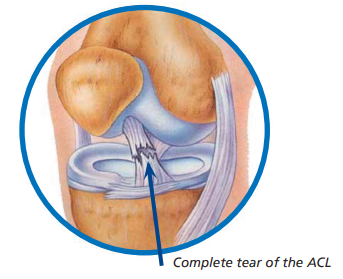
The knee joint is made of the femur (thigh bone), the tibia (shin bone) and the patella (knee cap).
The knee also has ligaments (these join bone to bone) that help to stabilise the joint. These include your PCL (posterior cruciate ligament) and ACL (anterior cruciate ligament). These cross each other inside your knee joint.
The ACL is a broad, thick, band which stops the shin bone from sliding forwards from the thigh bone. It starts at the bottom of the thigh bone, passes down and forward, and attaches to the top of the shin bone.
The PCL is a strong thick band which stops the shin bone from sliding too far backwards from the thigh bone. It starts at the back of the shin bone and attaches to the inside part of the thigh bone.
The most common causes of ACL injuries are:
- a direct blow to the knee
- coming to a sudden stop or slowing down very quickly (sudden deceleration) if you are, for example, running
- bending your knee too far backwards (hyperextension)
- twisting. For example, this might be from changing direction suddenly when you are moving or or when landing from a jump. This ‘pivoting can cause ‘rotational stress’ to your knee.
Muscles also play a vital role in supporting the knee. These include your:
- front thigh muscles (quadriceps or ‘quads’)
- back thigh muscles (hamstrings)
- calf muscle (gastrocnemius)
What happens if I have a ‘tendon graft’ operation?
The surgeon may use muscle or tendon from your own body to create a graft to rebuild the ACL. This is called an autograft.
This tissue usually comes from one of:
- the patella tendon (the tendon that connects your kneecap to your shin bone)
- the quadriceps tendon (the tendon that connects your thigh muscle to your kneecap)
If you have a patella or quadriceps graft, the surgeon will remove the middle third of the tendon to make the graft.
- the hamstring (muscles at the back of your thigh)
If your surgeon uses a hamstring graft to rebuild your ACL they will take a part of your hamstring muscle called the semitendinosus or your gracilis muscle (a long, thin muscle in your inner thigh). Sometimes they will take a part from both. They will then carefully stitch them together to make the graft.
For some people, depending on their injury and how their own tendons and muscles are, it may be better to have a graft which uses tendon tissue from a donor. This is called an allograft.
Your surgeon will always talk with you about whether they think it is better for you to have an autograft or an allograft before you have your operation. They will help you to decide which graft will give you the best outcome.
Whichever type of graft you have, small tunnels are drilled into your tibia (shinbone) and femur (thighbone). The graft is pulled through these and secured in place as close as possible to where your ACL was. The graft does the work that your damaged ACL used to do.
After your operation
Will I be in pain?
You may have some pain and discomfort after your operation.
Do : tell a doctor or nurse on the ward if your pain relief is not working. When you leave hospital we will give you painkillers to take home.
If you are in pain in the first few days after your operation make sure you are taking your pain medication. If you are still have pain when you are taking your pain medication try applying cold packs (ice pack or frozen peas wrapped in a damp towel inside a plastic bag) to the sore area for up to 15 minutes, every few hours. This can provide short-term pain relief. Do not get your dressing wet.
Be aware
– the ice must never be in direct contact with your skin
– avoid getting your wound dressing wet as this can increase the chance of wound infection.
My scar site is numb. Is this usual?
It is usual to have some loss of feeling around the cut in your skin made during your operation. This will usually improve slowly over time. Some numbness can remain long-term.
Will I have swelling?
Yes, it is usual to have swelling after your operation but too much swelling will slow your recovery.
To reduce the amount of swelling in your knee:
Do:
- rest often
- raise your leg at regular intervals throughout the day and whenever you are sitting down (unless you are doing your exercises). For example, sit with your leg up on a sofa or footstool. This is most important in the first 72 hours (3 days) after your operation.
Do not:
- rest all of the time. Aim for short periods when you are active.
- walk or stand around for too long (over 20 to 30 minutes) at a time
Can I put weight on my knee?
Most people are allowed to fully weight bear, but the physiotherapist will tell you if you are not allowed to put weight on the knee. This will vary depending on your surgeon’s instructions.
We may will give you a knee brace or splint to wear. This limits the movement of your knee. We will also give you crutches to aid your walking.
How long will I be in hospital?
Most people leave hospital one or two days after the operation. This gives you time to fully recover from the anaesthetic and have a session with the physiotherapist.
Can I drive?
When leaving the hospital, you will not be able to drive home.
Do:
arrange your own transport or take public transport. If you take public transport, a responsible adult should come with you to see you home.
You should not return to driving until:
- you are no longer needing walking aids
- you have stopped wearing your brace
- you can safely deal with all emergency situations without being in pain or hesitating. For example, you must be able to stop the car quickly and in full control (do an emergency stop) and safely avoid obstacles
- you are covered by your insurance company.
Be aware
always try driving in a safe place first.
Wait until your check-up with your surgeon or consultant and talk with them about whether you are fit to return to driving.
Leaving Hospital
If you leave hospital on the same day as your operation, someone should stay with you for 24 hours afterwards.
When can I return to work?
You may be able to do light duties after 2 weeks.
Be aware
you are likely to still be walking on elbow crutches and may still be wearing a knee brace. This may limit what you can do at work. You will also need to keep your leg raised up regularly throughout the day.
You may return to:
- desk-based work 3 to 4 weeks after your operation
- light manual work 6 weeks after your operation
- heavy manual work 3 to 4 months after your operation.
Your physiotherapist will guide you on when is the right time to return to work and what you are able to do at work.
After your operation your graft becomes weaker before it gets stronger again. It is at its weakest 6 to 12 weeks after your operation. You may need to change your duties at work to fit in with this.
How do I care for my wound and graft at home?
Before you go home from hospital (are discharged) the nurses will advise you on your:
- compression bandage and how long you will need to keep it on to reduce the chance that you may get a blood clot.
- stitches. If you have stitches which need to be removed, the nurse will tell you when this should be done. Not all surgeons use stitches to close an operation wound.
- stitch removal is usually done at your GP surgery
- you must arrange a ‘wound check’ appointment with your GP surgery as advised by the nurse.
At this appointment, which is usually 10 to 14 days after your operation, your stitches will be either trimmed or removed.
Washing or showering?
Keep your wound dry and clean. We recommend you to ‘strip wash’. This is the best and safest way for you to keep clean.
Follow the advice below when you are washing or showering:
Do:
- sit down on a plastic stool while you shower.
- hold your leg completely straight if you remove your splint or brace to wash or shower. You must do this until you have put your brace and splint back on.
- take extra care, especially in the shower, when your graft is at its weakest. This is usually between 6 to 12 weeks after your operation.
Do not:
- stand on a wet surface. If you do this and slip, it could damage the graft.
- let your wound get wet. This can lead to infection.
Will I have a follow up appointment with my orthopeadic surgeon?
Yes. Your surgeon will arrange for you to have a follow-up appointment with them. Your first appointment will usually be 2 to 3 weeks after your surgery.
Are there any symptoms that I could develop after my operation which mean I should contact my GP surgery or go to A&E?
Yes. Do contact your GP or go to your nearest A&E department If you have any of these symptoms:
- your knee becoming more swollen, hotter or redder (skin redness may appear differently in black or brown skin).
- new numbness or tingling in your foot or your foot changing colour
- temperature above 37°C
- oozing wound
- persistent pain or swelling in your calf or shortness of breath
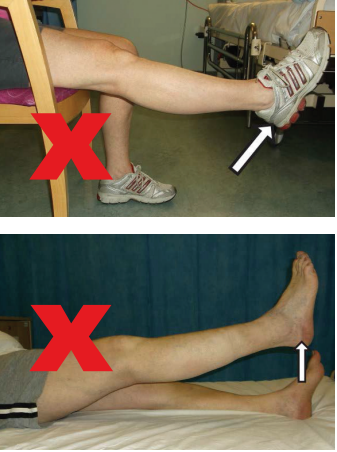
What movements should I avoid?
The following movements may put a strain on your graft and delay healing. Avoid doing these until your outpatient physiotherapist or consultant advises you that it is ok to do them. This is usually for about 2 weeks.
• Twisting, pivoting or turning abruptly on the operated leg.
• Lifting your leg or knee against gravity.

Will I have a Brace?
Before you go home, a physiotherapist may fit you with a brace. This will depend on whether your surgeon thinks this is right for you.
Do:
- continue to wear this until you are advised to remove it by your physiotherapist or surgeon. This is likely to be a minimum of 2 weeks.
- wear your brace all the time (day and night) except when you remove it to wash or dress.
The physiotherapist will ‘lock’ your brace when they fit it. This is so that it only allows you to move your knee as much as your surgeon has said is safe for you.
Do not:
- alter the setting to change this ‘range of movement’ unless your surgeon or physiotherapist tells you to do so.
After the physiotherapist has fitted your brace for the first time, it is easy for you to put it on and take off. To do this, open the Velcro straps and then the foam pads underneath.
When you take the brace off to wash or shower do hold your leg straight until you put your brace back on.
How should I use my crutches?
Follow this sequence when you walk using your crutches:
- move your elbow crutches forward first.
- then step your operated leg up to the crutches.
- step your non-operated leg forwards.
To go up and down stairs using your crutches follow the ‘ABC’ sequence:
- Up – Able leg, Bad leg, Crutches
- Down – Crutches, Bad Leg, Able Leg


When can I go the gym or return to doing sports?
You will not be able to go to the gym or swim for at least 2 weeks after your operation. You should wait until you see an outpatient physiotherapist. They will guide you as to when you are ready to begin specific activities.
Do not:
return to sport too soon. If you do, you may injure your knee again and it could mean that your replacement ligament fails. Your consultant and outpatient physiotherapist will advise how and when you can start training for sport again.
If you are making good progress this may be around:
- 5 to 6 months after your operation for non-contact sport
- 9 to 12 months for contact sport.
Physiotherapy
What must I do to help my own recovery?
The physiotherapy team and hospital staff will help you with your rehabilitation, but you need to help your own recovery by:
- managing your pain and swelling
- doing regular exercise as you have been advised
- following the advice in this information and that you are given by your surgeon and physiotherapy team.
What goals for my recovery should I aim for before and after my operation?
Your main goals should be to:
- be able to fully straighten your injured leg (achieve full extension of your leg)
- walk in the same way as you did before your injury and operation.
Other goals are to:
- minimize pain
- reduce swelling
- develop good strength and control in your front thigh muscles (quadriceps)
What exercises should I do to help me to recover and meet my goals after my operation?
There are different exercises that you should do at different stages of your recovery. At all stages of your recovery (stages 1 to 5)
Be aware
– people recover at different rates, and you may not be ready to do the exercises or activities shown for a stage as soon as the stated number of weeks after your operation.
– the exercises listed for each stage show examples of what some, but not all, people may be able to do during that stage.
– your physiotherapist will give you the exercises that are right for you at different stages of your recovery.
Stage 1 exercises (weeks 0 to 2)
Do these from straight after your operation until until the end of the 2nd week after your operation.
Do:
- tart these exercise straight away
- do them at least 3 to 5 times a day
- stop doing any exercises that are causing you too much pain (it is unlikely that they will) and contact the physiotherapy department for advice.
Do not:
- add any of your own exercises. Only do the exercises shown below.
1. Ankle pumps. It is important that you help the blood to circulate well in your lower legs. This is to reduce the chance that you may get a type of blood clot called a deep vein thrombosis (DVT).
- Push your foot down and away from you (point toes) Then bring your toes up towards your shins (flex your ankles). Repeat 10 times, 5 times per hour. Continue this exercise for the next 3 days.

2. Calf stretch Sit up in the bed with your legs out in front of you. Put a towel around your foot. Gently pull your ankle towards you and feel the stretch in your calf. Hold for 30 seconds. Repeat 3 times in a row.

3. Static quads: Sit or lie with your leg straight and then contract / tighten your quads (front thigh muscles) as hard as you can by pushing your knee downwards. Hold for 5 seconds and then relax. Repeat 10 times.

4. Knee bend (flexion) lying down. Lying on your back, slowly bend and straighten your operated leg. Make sure that the movement is smooth and that your foot is touching the bed all the time. Bend your knee as far as is comfortable or as far as your brace allows. Repeat 10 times.

5. Muscle tightening (co-contractions) lying on your back. Place a small towel roll under your operated knee. Push your heel down into the bed to get your hamstring muscles working. At the same time, push the back of your knee onto the towel roll to tighten your quadriceps muscle. Hold for 5 to 10 seconds and then relax. Repeat 10 times.

6. Moving your kneecap. Lie or sit with your leg straight and relaxed. Gently move your kneecap from side to side with your fingers as shown in the picture. Repeat 10 times.

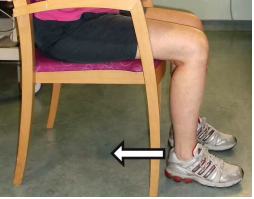
7. Knee bending (flexion) sitting down. Sit on a chair with your feet on the floor. Bend your knee as far as is comfortable or as far as your brace will allow. Then straighten your leg. Make sure that the sole of your foot is on the floor all of the time. Repeat 10 times.
8. Straighten and stretch sitting down. Sit on a chair, with your operated leg supported as shown. Relax and let the knee straighten with gravity. Stay in this position for 2 to 5 minutes. You can also do this exercise lying down on your bed. Place a rolled up towel underneath your heel and then relax your leg.

9. Hamstring stretch Sit on a chair with your operated leg straight and your heel resting on the floor. Lean forwards keeping your back straight until you feel a stretch along the back of your leg. This exercise can also be done sitting in bed. Stretch your operated leg out in front of you and reach forwards towards your toes. Hold for 30 seconds.

10. Hamstring curl Stand and hold on to a stable surface. Bend your operated knee to lift your foot slowly off the floor. Bend your knee as far as is comfortable or as far as your brace will allow. Slowly lower the foot back down. Repeat 10 times.

What can I expect from my ongoing physiotherapy rehabilitation?
Be aware
rehabilitation after you have had your ACL rebuilt is slow. The amount of exercise and physiotherapy that you need to get a good result can be intense. As well as regular physiotherapy reviews, you will need to continue exercising on your own for some months.
It is very important for you to play your part in your own recovery.
You will:
- have outpatient physiotherapy after you are discharged (go home) from hospital
- progress through a staged exercise and recovery programme designed to help people to recover from having an ACL rebuilt. Your physiotherapist will guide you through the exercises that you can do at each stage of your healing.
Do your exercises:
- as often as you have been advised
- in the way that you have been shown.
An outpatient physiotherapist will see you at your local physiotherapy department around 2 weeks after you leave hospital. They will:
- check how much you can move your knee (your range of movement)
- check that you are doing your exercises in the right way
- give you a new exercise programme to follow.
Outpatient Physiotherapy may involve:
- working on you getting full range of movement of your knee
- making the muscles around your knee (your quadriceps and hamstrings) stronger
- working towards you being able to walk as you could before your injury as far as possible. This includes helping you to be able to walk without your crutches.
- working on your balance and how agile you are
- training to help you to do sports and other activities
- helping you to return safely to work and doing sports.
If you do not receive an appointment for outpatient physiotherapy around 1 week after you have left hospital then please contact your local physiotherapy department. If they are unable to help then please call the inpatient physiotherapy department.
Stage two (early stage) exercises (2 to 6 weeks)
The aim is that by the end of stage two you gain full range of movement of your knee (can bend and straighten your knee fully).
Be aware
do not move on to doing these stage two exercises until your outpatient physiotherapist has advised you that you should.
During this stage:
- you should continue with your stage one exercises. You can add weights to these if your physiotherapist has advised you to.
- you can do more exercises to build up your strength and improve your balance.
- most people can start doing everyday things such as walking, standing, using stairs and getting in and out of a car again.
Use a static (exercise) bike
Spend less than 10 minutes on a bike. Set it to ‘low resistance’. To start with, you may find it easier to cycle backwards.
Squats
Stand with your feet shoulder width apart then slowly squat. To start with only go for a ¼ squat, then progress to a ½, ¾, and full squat as you are able to. Use a chair behind you to help check the depth of your squats. You may be able to move on to holding weights while you are doing squats if this is right for you.
Step ups and step downs
With a step in front of you, step up. Lead with your operated knee and then step down leading with your other knee.
Balance Exercises
Stand on your operated leg only. Aim to do this for 1 minute. If you would like to build on this exercise, try throwing and catching a ball against a wall at the same time.
You can also try walking in a straight line with a heel to toe walking pattern to improve your balance.
Stage three (mid-stage) rehabilitation (6 weeks to 3 months)
Be aware
do not move on to doing these stage 3 exercises until your outpatient physiotherapist has advised you that you should.
The aim in stage three is to:
- maintain your knee range of movement
- increase your strength exercises
- make your balance exercises more of a challenge for you.
You can now progress with all your strength training. Keep doing your stage two exercises and start using gym equipment.
Lunges:
Place your operated foot in front of you and lunge forward. Start with a ¼ lunge first. Move on to a full lunge as you are able to. Progress further by lunging onto a wobble cushion.
Balance exercises:
- Continue with single leg balancing. Increase the length of time you are able to balance for until it is the same on each leg
- Stand on a wobble cushion, throwing and catching a ball
- Sitting down and standing up on one leg.
- Trampet work, single leg balance, marching, jogging
- Hopping. Start by hopping on the spot, then forwards, backwards, sideways
Swimming
You can start swimming during this stage, but only if your wound has healed. Only do strokes that involve straight kicking.
Do not:
- do breast stroke.
Skipping
Start by skipping on two feet then progress to alternate feet
Treadmill
Walking forwards and backwards on the treadmill, slowly increase the pace. Work towards a slow jog by the end of this stage.
Cross trainer and rowing machine
Start with minimal resistance.
Stage four (late stage) rehabilitation (3-6 months)
Be aware
do not move on to stage four until your outpatient physiotherapist has advised you that you should.
The aim of stage four is to:
- maintain your range of movement
- progress your strength and your control of your body
- improve your balance through more advanced exercises
- start jogging.
Stage five – returning to Sport (6 to 9 months)
Be aware
do not move on to stage five until your outpatient physiotherapist has advised you that you should.
You may now consider returning to your chosen sport if you have:
- full range of movement
- no swelling
- good strength and stability of your knee
Working with your Physiotherapist, you may be able to return to training for your chosen sport. Progression should be staged from ¼ to ½ to ¾ to full intensity.
By the end of this stage your strength and control in the leg that you injured should be equal to that of the other side.
Further reading
Contact Details
If you have any urgent concerns about your exercises after you have read this information and before you see your out-patient physiotherapist, please phone the
![]() SOTC Physiotherapy department
01444 441881
Ext. 68834
SOTC Physiotherapy department
01444 441881
Ext. 68834
This leaflet is intended for patients receiving care in Haywards Heath.
The information in this leaflet is for guidance purposes only and is in no way intended to replace professional clinical advice by a qualified practitioner.
Today’s research is tomorrow’s treatments. That’s why UHSx is proud to be a research-active Trust. Find out how you can get involved.
Visit our website www.uhsussex.nhs.uk/research-and-innovation/information-for-patients-and-public or scan the QR code: 