Download and print as a PDF (708kB pdf)
Patient notes:
Weight Bearing Status:
Additional notes from your therapist:
What is this information about?
This information is about an operation called a total ankle replacement, or TAR. It explains what happens during a TAR operation, the possible risks of this operation, and what to do while you are recovering at home.
Why have I been given this information?
You, or someone you care for, has had a TAR. Reading this information, and following the instructions and advice here, will help you to know what to expect, and your recovery.
It also lists symptoms that need to be checked by a medical professional. Keep this information in a safe place, so that you can refer to it when you need to.
Why do I need a total ankle replacement?
Ankle replacements are done to treat arthritis which causes pain in the ankle. This pain cannot be controlled by other things like painkillers, shoe inserts, physiotherapy or using a walking aid.
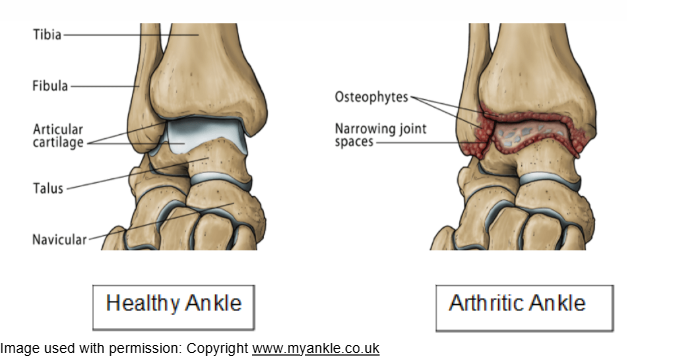
Arthritis is damage to one or more joints within the body. The most common type of arthritis is Osteoarthritis. This involves gradual wear and tear of the cartilage between the bone ends. This causes stiffness and increasing pain. In some people this type of arthritis can occur following an ankle fracture.
Other types of arthritis are caused by inflammation within the body, which leads to severe joint damage. This includes Rheumatoid Arthritis.
In either case the cartilage is destroyed within the joint. This causes the bones to rub together and causes pain and stiffness.
What is a total ankle replacement?
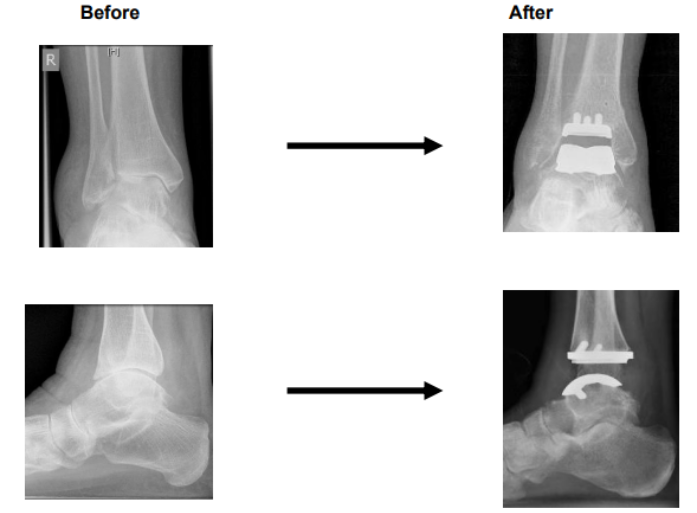
A total ankle replacement involves taking out the worn-out ends of your tibia and talus bones (two bones that form the main hinge in your ankle) and replacing them with artificial ends made from metal with a plastic insert. This is called a prosthesis.
Unlike an ankle fusion, a replacement allows you to move your joint after surgery.
Appearance on X-ray before and after the surgery
What are the benefits of the operation?
In most cases a replaced ankle will have the same range of movement that it had before the surgery. This means that you can walk normally.
There may also be less risk that you put strain on joints near your ankle once you have had an ankle replacement.
Research shows that if patients follow recovery instructions after an ankle replacement operation, about 90% feel less pain, move more easily, and enjoy a better quality of life.
Studies also show that 85 to 90% of ankle replacements still work well 10 years after the operation.
What are the risks of the operation?
All surgery and anaesthetics carry some risks, especially if you have other medical problems, smoke, or are overweight.
The healthcare team looking after you have been trained to reduce these risks and make sure that your treatment is safe.
The risks include:
Infection
Sometimes, even after being very careful, infections can happen. These need to be treated with antibiotics.
Infection can be:
- Superficial (surface) infection that can happen at your wound site.
- Deep infection that may happen early after the operation or much later. This is rare (less than 1%)*
To help reduce the risk of infection
Do
- keep your wound dry
- tell your GP as soon as possible if you feel generally unwell or have a temperature. An infection in one area of the body can spread and cause problems in your ankle.
- give up or at least cut down if you are a smoker. You are more likely to get an infection if you smoke.
Wound healing problems
Wound healing problems can happen if you:
- Have a chronic illness such as diabetes or rheumatoid disease
- Are taking some medicines that affect the immune system (The approximate risk is 1 in 8)*
- Are a smoker. We strongly advise you to give up or at least cut down.
Loosening of the prosthesis (new joint)
This is a risk of all artificial joints. It is caused by a weakening of the bond between the new joint and your bone.
Hopefully your new ankle will last at least 10 or more years, but it may loosen before this time. This is more likely to happen if you:
- are overweight
- damage the joint by falling on it
- return to heavy employment.
If it does loosen then it can be possible to remove it and replace it with another one. This is a more complicated operation with greater risks.
If the ankle replacement fails, it is often treated by ankle fusion (fusing the bones together), usually with a bone graft. This is usually successful but is a more complex operation. It also has higher risks than a primary (first time) ankle fusion.
The risk of needing a revision total ankle replacement is 15% at 10 years*.
Ankle fracture
There is a small risk of fracture of the ankle during the operation as well as after the operation. This risk is about 1 in 25*.
Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE)
Even after being very careful, blood clots in the veins of the legs (DVT) can sometimes happen after this type of surgery.
Occasionally these clots can dislodge and travel through the heart to the lungs. This is known as a pulmonary embolism (PE). This can be life-threatening, but it is very rare.
Pain and stiffness that continues after the operation
The operation may not get rid of all of your pain. You may continue to feel some mild discomfort.
Complex regional pain syndrome is uncommon but it may be the cause of pain, swelling and skin changes.
Your ankle can become stiff after surgery. We encourage you to do physiotherapy exercises to help with this.
Nerve Damage
Very occasionally nerves can be damaged or stretched during your operation. This usually recovers over a period of time.
Other recognised risks of surgery include bruising, urinary retention and the risks associated with anaesthesia. (Approximate risk 1 in 23)*.
Amputation
There is a risk that the ankle replacement could fail completely, especially if there is a severe infection that cannot be fully cleared. If this happens, it may be necessary to have an amputation. This risk is approximately 1% (1 in 100).
When will I go home?
Unless told otherwise by your foot and ankle consultant, you will normally stay in hospital overnight and go home the day after your surgery. Some people may be able to go home the same day.
Do I need to plan how to manage when I return home?
Yes. It is important that you plan how you will manage at home after your operation, as will not be able to move around easily.
You may need to organise for someone to stay with you, or to bring a bed downstairs if you feel that you will struggle to manage the stairs after your surgery.
If you feel you will struggle after surgery, please contact our Occupational therapy team to discuss this on 01444 441881 ext 68866.
Will it be painful?
It is normal to have some pain and discomfort in your ankle after replacement surgery.
When you wake up after the surgery your ankle will be numb. This is because during the surgery you will have a special pain block performed, called a popliteal block. This will last 12 to14 hours. After this you will need to make sure that you are taking effective pain relief, which the doctors will prescribe for you.
Make sure you let the nurses know as soon as you feel pain, so they can help you to get it under control. It is harder to control pain if you let it build up to a level that you cannot manage.
It is important to make sure that you take enough pain relief to keep your ankle moving, and to allow you to safely mobilise (walk with aids).
Do not take anything which is not on your prescription, and make sure you take your pain relief as directed to do so. If you run out of pain relief, then contact your GP.
What is Deep Vein Thrombosis (DVT)? What can I do to help reduce the risk?
A risk of total ankle replacement surgery is DVT. DVT is a clot that can form in the deep veins in your leg following surgery. DVT tends to mainly affect the lower leg or calf, but can form in other veins too.
There is a slightly higher risk of developing DVT following total ankle replacement surgery, so it is important to be aware of and notice any problems.
Be aware
Seek immediate medical advice by calling the GP or 111 if you experience any of the following symptoms:
– throbbing or cramping pain in 1 leg (rarely both legs), usually in the calf or thigh
– swelling in 1 leg (rarely both legs)
– warm skin around the painful area
– red or darkened skin around the painful area
– swollen veins that are hard or sore when you touch them
Call 999 or go straight to A&E
If you have the above symptoms of a DVT and get:
- breathlessness
- chest pain
To help reduce the risk of DVT you may be prescribed some special medication in the form of an injection or tablet. The nurses will show you how to use this before you go home.
Do
- Keep hydrated (drink enough).
- Practice your physiotherapy exercises prescribed later in this booklet.
- Keep mobile (move around). This means not spending all day resting in bed. Try to get yourself up and sit in a chair with your leg elevated (raised up) in between rest periods.
What can I do to help my recovery?
After ankle replacement we recommend you follow the RICE advice. This stands for Rest Ice Compression and Elevation.
Rest:
Although it is essential to keep moving, it is also important that you rest to begin with, especially during the first 10 to 14 days.
Try to balance rest and movement. Avoid any unnecessary activity. If you are able to, rest indoors for the first 10 to 14 days, then slowly and gradually build up walking outdoors when you feel ready.
An increase in pain can sometimes indicate that you are overdoing things, so be guided by how your ankle feels and reduce activity if you need to.
Ice:
You can start to use ice therapy after 2 weeks, once the dressings have been removed. Ice can be good for pain relief and swelling.
A bag of frozen peas, wrapped in a damp towel and placed inside a plastic bag makes a good ice pack or you may use the gel-type ice packs.
Place the ice pack on the ankle for up to a maximum of 20 minutes at a time, every hour if needed. Make sure to regularly check your skin to make sure that you do not get an ice burn.
Compression:
You may go home with a crepe bandage on your ankle. This provides compression and helps to reduce swelling. The nurses will advise you how long this must remain on for. This is usually 24 to 72 hours, but this depends on what your surgeon thinks.
Elevation:
Elevating (raising up) your leg will help to reduce swelling. Make sure when you are sitting that your leg is elevated. The following points are important:
- Your leg is held straight when elevated
- Your foot is above hip level
- You have support along the whole leg (not just your foot).
Exercises:
Little and often is best. Aim to do the exercises regularly throughout the day rather than doing one big set.
Start by doing as many repetitions as you can manage, using the numbers indicated as a guideline. Gradually increase the repetitions as the exercise becomes easier. None of the exercises should cause excessive pain.
Be aware
If any particular exercise causes pain, stop doing it and contact the physiotherapist for advice.
What exercises do I need to do?
The following exercises need to be done from the first week.
Deep breathing exercises
Ensure you are sitting upright in bed. Take three or four deep breaths (no more as you may feel lightheaded). Breathe as deeply as possible and hold each breath for 3 to 4 seconds. This may make you cough.
Ankle pumps while you are lying on your back
- Lie on your back with your legs straight.
Briskly bend and straighten your ankles. - Repeat 10 times, hourly.

Toe Flexion and Extension
- Bend and straighten your toes.
- Use your fingers to assist if necessary.
- Repeat 10 times, 3 to 5 times a day

Will I be given a walking boot?
Most people will need to wear a boot on the operated leg. Your physiotherapist or nurse will give you this and teach you how to put on, take off, and manage your boot.
The foot and ankle consultant will decide when you will start wearing the boot.
If your ankle is very swollen, they may decide to put you in a below-knee plaster until your clinic review at 2 to 3 weeks. This will then be swapped for a fresh plaster or boot. However, most people will be in a boot immediately following surgery.
Types of boot:


How should I wear the boot?
When wearing the boot, it is important that it is applied correctly so that your heel is back in the boot and your foot is flat.
You must take it off every day for hygiene and wound inspection purposes, and when dressing and undressing. Take time while the boot is off to check the skin around your ankle for pressure sores. If you are concerned, please contact the ward staff while you are an inpatient, or the foot and ankle consultant or your GP when at home.
The boot can be wiped clean with a damp cloth. The soft inner liner can be washed in a mild soap solution.
For the first three weeks after your operation, the boot must be worn for 23 hours per day.
Do not
- walk without the boot.
From week four until your follow up appointment with your Surgeon (4 to 8 weeks), the boot must be worn when walking but can be taken off at rest.
Do not
- walk without the boot.
If you have any problems or queries regarding the boot, please contact the physiotherapy department, especially if the boot feels too loose once the swelling has gone down after your operation.
Walking
A little walking is important to help reduce the risk of problems after the operation, like DVT and chest infection.
For the first 10 to 14 days we recommend that you only do what is necessary. You can then gradually increase the distance that you walk as long as you are comfortable to do so.
You may have been given crutches or a zimmer frame to help you. You will have been told how much weight (if any) you are allowed to put through your operated leg. This is called your weightbearing status.
You must continue to use the walking aid and keep to your weightbearing status until your foot and ankle consultant or physiotherapist gives you different instructions.
Should I stop smoking?
Yes. Smoking seriously affects bone healing cells so that the wound and bones are less likely to heal; it also increases your chance of a chest infection after the anaesthetic.
You are strongly advised to give up or at least cut down drastically to help reduce this.
When can I start driving again?
You cannot drive until instructed by your surgeon or physiotherapist. This is normally for a minimum of 6 to 8 weeks but can be longer.
Before you start to drive you MUST be certain that you can control the vehicle and do an emergency stop. We suggest that you try sitting in the car and practising using the brake and gears before you drive on the road.
You should contact your insurance company to let them know that you have had the procedure and that you intend to return to driving to make sure that you are covered.
When can I return to work?
This will depend on your job.
- If you are in a sedentary job (a job where you are sitting down most of the time) you may return as soon as you feel able, usually after 3 to 4 weeks. Make sure that you can elevate your ankle while you are working.
- If your job is more active, you may need to be away for longer (6 to 8 weeks). You may also need a gradual return to work activities. Speak with your physiotherapist or your foot and ankle consultant about this.
When can I get back to leisure activities and sports?
Gentle non-contact activities or sports can be started after three months if your strength and movement have returned enough.
Very vigorous or impact-type exercise such as road running, football or squash are not advised at any stage after an ankle replacement.
Speak with your foot and ankle consultant or physiotherapist about any specific activity or sport that you enjoy.
How to use the stairs if you are weightbearing
It is fine for you to use the stairs. We advise that for the first couple of weeks that you take one step at a time, using the following method.
Be aware
If you are partial (PWB) or touch weightbearing (TWB) make sure to take your time. The physiotherapist will have told you whether you are PWB or TWB and explained what this means. If you are unsure, please check with them. Be careful to keep to your weightbearing status. Always go one step at a time.
Walking up stairs: ABC
- Hold onto the handrail (if you have one) with one hand and the crutches with the other hand.
- First take a step up with your healthy leg. ABLE (A)
- Then take a step up with your affected leg. BAD (B)
- Then bring your crutch up on the step. CRUTCH (C)

Walking down stairs: CBA
- Stand close to the stairs. Hold onto the handrail with one hand and the crutches with the other hand.
- First put your crutch one step down. CRUTCH (C)
- Then take a step with your affected leg. BAD (B)
- Then take a step down with your healthy leg, onto the same step as your affected leg. ABLE (A)

How to use the stairs if you are non-weightbearing (cannot put any weight through your operated leg)
Going upstairs:
- At the bottom of the stairs, take hold of the rail.
- Make sure that your elbow crutch is in the opposite hand.
- Carry your second elbow crutch up, position it in a ‘T’ shape.
- Make sure that your operated leg is bent up behind you.
- Leaning through your elbow crutch and the rail, hop up to the first step with your un-operated leg.
- Then bring your elbow crutch up to the same step.
- Repeat this pattern until you reach the top
- Move away from the stairs as soon as you reach the top.

Going downstairs
- At the top of the stairs, take hold of the rail on one side, and elbow crutch in the other (T-shape)
- Place the elbow crutch on the step below and bring your opposite arm down level.
- Hold your non-weight bearing limb in front of you.
- Gently lower your un-operated foot down on to the same step as your elbow crutch.
- Repeat until you reach the bottom.

Will I have any follow-up appointments?
Physiotherapy
Not all patients are referred to outpatient physiotherapy straight away. Sometimes your foot and ankle consultant will decide at your clinic appointment when it is best for you to start outpatient physiotherapy.
If you are referred for outpatient physiotherapy when we discharge you and do not receive an appointment after 3 weeks contact us on 01444 441881 ext 68834.
Foot and ankle consultant
The follow-up times can vary for different foot and ankle consultants. You will normally be seen at 1 or 2 weeks after your operation for a wound check. This may be with a nurse, GP, or your foot and ankle consultant.
A second follow-up will normally be arranged with your foot and ankle consultant between 4 to 8 weeks after your operation.
Who can I contact for further information and advice?
Physiotherapy rehabilitation information:
![]() SOTC Physiotherapy
01444 441881
Ext. 68834
SOTC Physiotherapy
01444 441881
Ext. 68834
![]() SOTC Occupational Therapy
01444 441881
Ext. 68866
SOTC Occupational Therapy
01444 441881
Ext. 68866
Further Resources and references
Ankle Replacement – The National Joint Registry Versus ArthritisThis leaflet is intended for patients receiving care in Hayward’s Heath.
The information in this leaflet is for guidance purposes only and is in no way intended to replace professional clinical advice by a qualified practitioner.
Today’s research is tomorrow’s treatments. That’s why UHSx is proud to be a research-active Trust. Find out how you can get involved.
Visit our website www.uhsussex.nhs.uk/research-and-innovation/information-for-patients-and-public or scan the QR code: 