Download and print as a PDF (1MB pdf)
What is Necrotising Enterocolitis (NEC)?
The aim of this leaflet is to answer some of the questions you may have about your baby’s stoma. If you have any further questions or concerns, please speak to a doctor or nurse caring for your baby.
What is a stoma?
A stoma is formed during surgery to make an opening on to the abdomen (tummy) which allows stool (poo) to flow out. A stoma might be performed on your baby for a number of reasons, and your nurse or doctor will help explain these reasons to you.
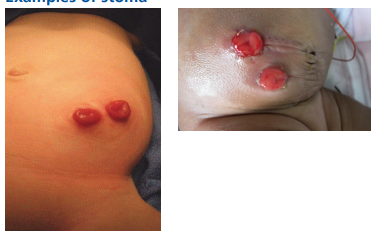
What does a stoma look like?
Stomas are made by using part of the bowel. Stomas are red, like the inside of your mouth, and are soft and moist. They have a good blood supply, so may bleed a little when they are touched. Stomas have no feeling so it will not hurt your baby when the stoma is touched.
Stomas can differ from baby to baby in size and shape. This means that your baby’s stoma may look different from pictures you see. Some stomas may protrude more than others and can be located on different areas on the abdomen.
Types of stoma
The most common types of stomas are a colostomy and an ileostomy.
A colostomy is a stoma that is formed from part of the colon which is also called the large bowel. When poo enters the colon, water is absorbed and the poo becomes drier, it is then passed out of the body via the stoma. The type of poo that comes from a colostomy can either be liquid or more solid in consistency.
An ileostomy is a stoma that is formed from the ileum, which is part of the small bowel. The ileum is earlier on in the digestive tract and contains digestive enzymes which help to break down food and aids absorption of nutrients from our diet. The type of poo that comes from an ileostomy is generally liquid or pasty in consistency.
In some cases, two stomas can be formed from the same area of the bowel. They are referred to as the proximal and distal stomas. The proximal stoma is the one that produces the poo, whilst the distal stoma (also known as the mucous fistula) is said to be non-functioning, but may produce mucous and gas.
The distal stoma may be used for a procedure known as ‘recycling’. Recycling involves putting back some of the poo into the distal stoma and is done to stimulate that part of the bowel which has not been working since the surgery. This may be done in preparation for an operation in which the stoma is reversed.
Following your baby’s operation, the surgeon will explain to you exactly what surgery your baby has had and whether a colostomy or ileostomy was needed.
What happens after my baby’s surgery?
After the operation, there is likely to be a small dressing over your baby’s wounds and stoma. At first, the stoma may not look as it was described earlier, and it is not unusual for the stoma to be slightly dusky in colour. It may also develop a scab due to bleeding that may have occurred after the operation. You may be able to see stitches, which will eventually dissolve on their own.
The nursing and medical team will keep a close eye on the stoma and surrounding skin and keep the area clean and dry. The nursing staff will also be monitoring for when the stoma begins to produce poo. This may happen within the first few days, or it may take longer, and this will depend on a) why your baby needed a stoma, and b) the type of surgery your baby has had.
Once the stoma is active, the nursing staff will put a stoma pouch over the stoma to collect the poo. There are many different types of stoma pouches and we may try a number pouches until we find the one that is best for your baby. If your baby has two stomas the distal (non-functioning) stoma will either be covered with a pouch, or it will have a dressing over the top of it.
How do I care for my baby’s stoma?
In hospital you will be shown how to look after your baby’s stoma. One of the first things that you will learn is how to empty the pouch. This is usually done by inserting a syringe and quill into the pouch and drawing the fluid out. The fluid is measured in the syringe to see how much poo has been passed. The inside of the pouch does not have to be cleaned once emptied, but it may be beneficial to wipe the end of the pouch to prevent any poo from getting on your baby’s clothing.
The pouch needs to be changed every 24-72 hours and if it is showing signs of leakage. When changing the pouch, you need to remove the pouch from your baby’s abdomen and then clean and dry around the stoma. When applying a new pouch, it is important to ensure that it fits snugly around the stoma, so that poo is prevented from going directly onto the skin. Your nurse and/or the stoma nurse specialist will show you how to do this.
When can I start feeding my baby?
Decisions about when to start feeding your baby will depend on why your baby has had a stoma formed and what type of stoma they have. Usually, feeding won’t start until the stoma is active, however it could be up to two weeks or even longer before milk can be given.
Monitoring stoma losses
Once you begin feeding your baby, the nursing staff will make notes on how much poo your baby is producing. This is particularly important if your baby has an ileostomy, as the poo can be very liquid in nature.
We will monitor to check that your baby’s output is less in volume than the milk they are receiving. This is important as it helps us to ensure that your baby is absorbing the nutrients that they need in order to grow.
Are there any potential complications?
The main potential complications of having a stoma are listed below:
Skin irritation
Although the stoma itself has no sensation, the skin surrounding it does and it can become irritated by both the adhesive on the stoma pouch, and also by the poo itself. Often, these irritations can be minor, but in some cases they can start to cause the skin to break down. The nursing staff and the stoma nurse specialists will observe for early signs of irritation and provide appropriate advice and care.
Prolapse
A prolapse is when the bowel becomes longer and protrudes through the opening of the stoma. Although this can be very frightening for parents, it is not usually serious. As long as the bowel remains pink and active, we will simply keep a close eye on it.
Retraction
Retraction of the stoma is when the stoma is below the skin level. This can lead to problems with applying the pouch. The nursing staff and stoma nurse specialists will have suggestions on how to help manage a retracted stoma.
Bleeding
The stoma will occasionally bleed, especially when touched; this is normal. However, if the bleeding does not stop or it is coming from inside the stoma then medical advice is required.
Hernia
Hernias are very common in premature babies. Surgery causes a weakness in the abdominal muscle wall allowing parts of the bowel to protrude which creates a bulge under the skin. A hernia can make pouch security more difficult. The nursing staff and stoma nurse specialists will provide advice to help manage a hernia.
Reversing the stoma
Reversing (closing) the stoma requires an operation with a general anaesthetic. Your baby’s surgeon will advise on when the stoma can be reversed. The length of time that your baby will need a stoma depends on the reason that the stoma was initially formed. Sometimes your baby will stay in hospital until after the stoma is reversed (closed). This is usually because they are unable to tolerate ‘full milk feeds’, meaning that your baby is not able to get his or her entire nutritional requirement through milk. If this is the case, the stoma will usually be reversed before going home from hospital. If your baby is able to go home from hospital with a stoma, the surgeons will inform you of future plans regarding stoma reversal.
Caring for my baby at home
Leaving hospital
In some cases you will take your baby home with a stoma. This may feel scary at first, but nursing staff will ensure that you are confident in caring for the stoma and that you have all the information and support you need before your baby is discharged home.
Clothing
Your baby will not need special clothes, but you should avoid clothes that may rub against the stoma, or prevent the pouch from filling. Similarly, your baby will not need special nappies. The nurse will show you how to apply the nappy over the stoma pouch.
Bathing
You can bathe your baby with the stoma pouch on or off. It is recommended that you avoid using oily soaps or lotions, as these can stop the pouch from sticking to the skin.
Contact details:
If you have any further questions, please ask one of the nurses or doctors on the Unit:
![]() TMBU
01273 696955
Ext. 64377
TMBU
01273 696955
Ext. 64377
![]() Stoma Care Department
01273 696955
Ext. 64215
Stoma Care Department
01273 696955
Ext. 64215
Support groups
Breakaway Foundation
Telephone 01283 240253 Email [email protected]
A Bear Named Buttony
Bears with stomas which are donated to children who have a stoma formed.
Telephone 07813 720963
Email [email protected]
Bliss
Premature Baby Charity
Telephone 0808 8010322
Email [email protected]
Ileostomy Association
Telephone 0800 0184724
Colostomy UK
Telephone 0800 3284257
This leaflet is intended for patients receiving care in Brighton & Hove or Haywards Heath.
The information in this leaflet is for guidance purposes only and is in no way intended to replace professional clinical advice by a qualified practitioner.